Suggest an improvement

var gform;gform||(document.addEventListener(“gform_main_scripts_loaded”,function()gform.scriptsLoaded=!0),document.addEventListener(“gform/theme/scripts_loaded”,function()gform.themeScriptsLoaded=!0),window.addEventListener(“DOMContentLoaded”,function()gform.domLoaded=!0),gform=domLoaded:!1,scriptsLoaded:!1,themeScriptsLoaded:!1,isFormEditor:()=>”function”==typeof InitializeEditor,callIfLoaded:function(o)!gform.themeScriptsLoaded&&!gform.isFormEditor(),initializeOnLoaded:function(o)gform.callIfLoaded(o),hooks:action:,filter:,addAction:function(o,r,e,t)gform.addHook(“action”,o,r,e,t),addFilter:function(o,r,e,t)gform.addHook(“filter”,o,r,e,t),doAction:function(o)gform.doHook(“action”,o,arguments),applyFilters:function(o)return gform.doHook(“filter”,o,arguments),removeAction:function(o,r)gform.removeHook(“action”,o,r),removeFilter:function(o,r,e)gform.removeHook(“filter”,o,r,e),addHook:function(o,r,e,t,n)null==gform.hooks[o][r]&&(gform.hooks[o][r]=[]);var d=gform.hooks[o][r];null==n&&(n=r+”_”+d.length),gform.hooks[o][r].push(tag:n,callable:e,priority:t=null==t?10:t),doHook:function(r,o,e)var t;if(e=Array.prototype.slice.call(e,1),null!=gform.hooks[r][o]&&((o=gform.hooks[r][o]).sort(function(o,r)return o.priority-r.priority),o.forEach(function(o)”function”!=typeof(t=o.callable)&&(t=window[t]),”action”==r?t.apply(null,e):e[0]=t.apply(null,e))),”filter”==r)return e[0],removeHook:function(o,r,t,n)var e;null!=gform.hooks[o][r]&&(e=(e=gform.hooks[o][r]).filter(function(o,r,e)),gform.hooks[o][r]=e));

-
N/AFix spelling/grammar issueAdd or fix a linkAdd or fix an imageAdd more detailImprove the quality of the writingFix a factual error
-
You don’t need to tell us which article this feedback relates to, as we automatically capture that information for you.
-
This allows us to get in touch for more details if required.
-
Enter a five letter word in lowercase
#gform_wrapper_38 .gform_footer visibility: hidden; position: absolute; left: -100vw;
-
This field is for validation purposes and should be left unchanged.
/* = 0;if(!is_postback)return;var form_content = jQuery(this).contents().find(‘#gform_wrapper_38’);var is_confirmation = jQuery(this).contents().find(‘#gform_confirmation_wrapper_38’).length > 0;var is_redirect = contents.indexOf(‘gformRedirect(){‘) >= 0;var is_form = form_content.length > 0 && ! is_redirect && ! is_confirmation;var mt = parseInt(jQuery(‘html’).css(‘margin-top’), 10) + parseInt(jQuery(‘body’).css(‘margin-top’), 10) + 100;if(is_form)jQuery(‘#gform_wrapper_38’).html(form_content.html());if(form_content.hasClass(‘gform_validation_error’))jQuery(‘#gform_wrapper_38’).addClass(‘gform_validation_error’); else jQuery(‘#gform_wrapper_38’).removeClass(‘gform_validation_error’);setTimeout( function() /* delay the scroll by 50 milliseconds to fix a bug in chrome */ jQuery(document).scrollTop(jQuery(‘#gform_wrapper_38’).offset().top – mt); , 50 );if(window[‘gformInitDatepicker’]) gformInitDatepicker();if(window[‘gformInitPriceFields’]) gformInitPriceFields();var current_page = jQuery(‘#gform_source_page_number_38’).val();gformInitSpinner( 38, ‘https://geekymedics.com/wp-content/plugins/gravityforms/images/spinner.svg’, true );jQuery(document).trigger(‘gform_page_loaded’, [38, current_page]);window[‘gf_submitting_38’] = false;else if(!is_redirect)var confirmation_content = jQuery(this).contents().find(‘.GF_AJAX_POSTBACK’).html();if(!confirmation_content)confirmation_content = contents;jQuery(‘#gform_wrapper_38’).replaceWith(confirmation_content);jQuery(document).scrollTop(jQuery(‘#gf_38’).offset().top – mt);jQuery(document).trigger(‘gform_confirmation_loaded’, [38]);window[‘gf_submitting_38’] = false;wp.a11y.speak(jQuery(‘#gform_confirmation_message_38’).text());elsejQuery(‘#gform_38’).append(contents);if(window[‘gformRedirect’]) gformRedirect();jQuery(document).trigger(“gform_pre_post_render”, [ formId: “38”, currentPage: “current_page”, abort: function() this.preventDefault(); ]); if (event && event.defaultPrevented) return; const gformWrapperDiv = document.getElementById( “gform_wrapper_38” ); if ( gformWrapperDiv ) const visibilitySpan = document.createElement( “span” ); visibilitySpan.id = “gform_visibility_test_38”; gformWrapperDiv.insertAdjacentElement( “afterend”, visibilitySpan ); const visibilityTestDiv = document.getElementById( “gform_visibility_test_38” ); let postRenderFired = false; function triggerPostRender() if ( postRenderFired ) return; postRenderFired = true; gform.core.triggerPostRenderEvents( 38, current_page ); if ( visibilityTestDiv ) visibilityTestDiv.parentNode.removeChild( visibilityTestDiv ); function debounce( func, wait, immediate ) var timeout; return function() var context = this, args = arguments; var later = function() timeout = null; if ( !immediate ) func.apply( context, args ); ; var callNow = immediate && !timeout; clearTimeout( timeout ); timeout = setTimeout( later, wait ); if ( callNow ) func.apply( context, args ); ; const debouncedTriggerPostRender = debounce( function() triggerPostRender(); , 200 ); if ( visibilityTestDiv && visibilityTestDiv.offsetParent === null ) const observer = new MutationObserver( ( mutations ) => mutations.forEach( ( mutation ) => if ( mutation.type === ‘attributes’ && visibilityTestDiv.offsetParent !== null ) debouncedTriggerPostRender(); observer.disconnect(); ); ); observer.observe( document.body, attributes: true, childList: false, subtree: true, attributeFilter: [ ‘style’, ‘class’ ], ); else triggerPostRender(); } );} );
/* ]]> */

Introduction
A haemothorax is where blood enters the pleural cavity and can be characterised by a pleural fluid haematocrit greater than 50%.1
A haemopneumothorax is defined as blood and air entering the pleural cavity.
The most common cause of haemothorax is trauma, with other causes including vascular pathologies, iatrogenesis, malignancy and blood clotting disorders.2
Aetiology
All causes of haemothorax involve major vessels in the thorax, including the intercostal arteries, aorta and internal mammary arteries.
Traumatic
Major incidents of trauma, which include blunt or penetrating injury, can cause a haemothorax as well as a haemopneumothorax.
Iatrogenic
Medical procedures can damage the major vessels in the thorax and the lungs. These include:2
- Chest drain insertion
- Central venous catheterisation (particularly subclavian)
- Needle decompression
- Thoracotomy
- Cardiopulmonary resuscitation
Spontaneous
Various conditions can lead to spontaneous haemothorax:
- Primary lung conditions: commonly caused by a primary pneumothorax
- Vascular pathologies: causing the rupture of the great vessels within the thorax (e.g. ascending aorta). Primary connective tissue diseases, such as Ehlers-Danlos and Rendu-Osler-Weber syndrome, cause changes to the vascular structure
- Coagulopathies: predisposing to bleeding into the thoracic cavity (e.g. haemophilia and thrombocytopenia)
- Malignancy: can invade surrounding vasculature and lead to haemorrhage (e.g. mesothelioma)2
Pathophysiology
In health, both alveolar and atmospheric pressures are greater than the intrapleural pressure. This creates a pressure gradient that aids in the ventilation of the lungs.
When bleeding occurs into the pleural cavity, intrapleural pressure increases and thus, the pressure gradient decreases, reducing ventilation.
Hypoxia and haemodynamic instability are further worsened by blood loss into the pleural cavity, and intrapleural blood loss can exceed 1.5 litres.3
Clinical features
History
Symptoms of haemothorax include:
- Worsening shortness of breath
- Ipsilateral pleuritic chest pain
- Non-productive cough
- Chest wall bruising
Clinical examination
Typical signs of haemothorax include:
- Dullness to percussion
- Reduced/absent breath sounds
- Tachypnoea
- Tracheal deviation (away from the affected side)
- Hypoxia
- Hypovolaemic shock
- Flail chest

Investigations
Bedside investigations
Relevant bedside investigations include:
- Basic observations: may show hypoxaemia and tachypnoea, with hypotension and tachycardia in hypovolaemic shock
- Arterial blood gas: if hypoxaemic, to assess ventilation and gas exchange
Laboratory
Relevant laboratory investigations include:
- Full blood count: may show anaemia secondary to blood loss
- Coagulation screen: to identify bleeding disorders
- Group and save/crossmatch: in preparation for blood transfusion
- Pleural fluid sample: for microbiology (culture and gram stain), biochemistry (protein, haematocrit and glucose) and cytology (underlying malignancy); sample can tested using a blood gas analyser to quickly determine the haematocrit
Imaging
Relevant imaging includes:
- Thoracic ultrasound: point-of-care imaging showing heavily echogenic fluid within the pleural space
- Chest X-ray: costophrenic blunting, meniscus sign and mediastinal shift in larger haemothoraces.4 It cannot distinguish between a haemothorax and other causes of a pleural effusion
- CT thorax: to identify other injuries or causes of haemothorax and can also determine the attenuation valve of the fluid, aiding identification. CT angiogram can detect the site of bleeding aid management

Differential diagnoses
Relevant differentials for haemothorax include:
- Tension pneumothorax: may also present with haemodynamic instability and mediastinal shift. Tension pneumothorax can be differentiated from a haemothorax through percussion; tension pneumothorax will be hyper-resonant, whereas haemothorax will be dull
- Pleural effusion: may present alongside or separately from haemothorax in cases with a more chronic onset. Definitive differentiation is made by pleural fluid aspiration. Malignant pleural effusions may look very similar to that of a haemothorax, but a comparison of haematocrit concertation can aid diagnosis (greater than 50% to confirm a diagnosis of haemothorax)
Management
In suspected cases of haemothorax, an ABCDE approach should be used, and emergency management should be commenced (e.g. fluid resuscitation or blood transfusion).
The treatment of a traumatic haemothorax can be split into treating the haemothorax and treating the primary haemorrhage.
Haemothorax treatment
Patients with large haemothoraces require chest drain insertion under ultrasound guidance. Bubbling during insertion may indicate a haemopneumothorax.2
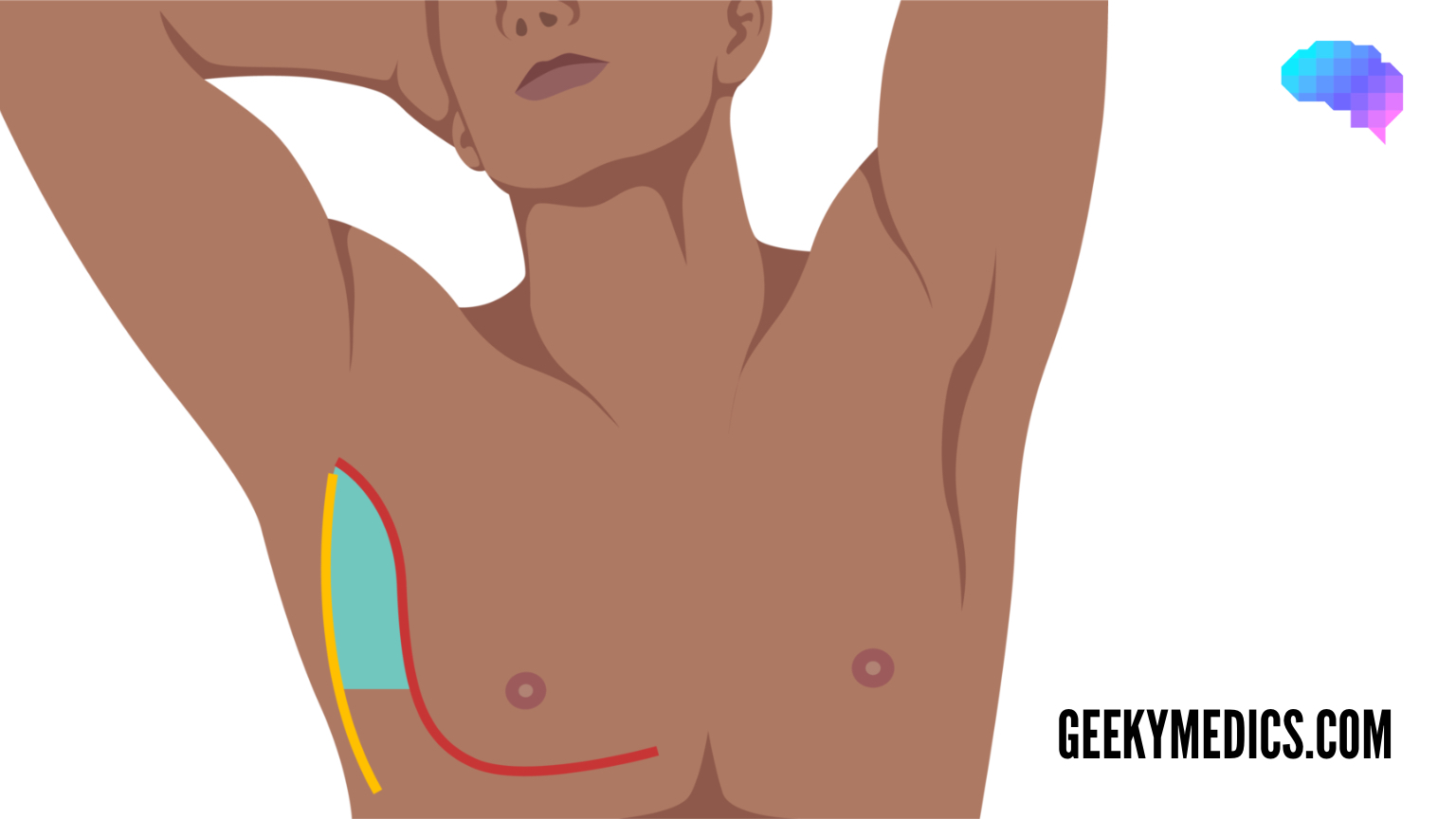
Chest drain insertion
Intercostal drains are typically inserted into the triangle of safety. This is the space between the fifth intercostal space, midaxillary line and anterior axillary line.
To avoid the neurovascular bundle below each rib, the chest drain needle should be inserted directly above the rib.
Blood, pleural fluid and air can exit the system into the chest drain collection bottle, and the volume of blood can be measured.6
Primary haemorrhage treatment
Treatment of the primary haemorrhage is essential for non-resolving haemothorax. Video-assisted thoracic surgery or a thoracotomy can be used to identify and resolve the underlying bleed.2
Interventional radiology can use an endovascular transcatheter to embolise or insert a stent graft into the site of arterial injury.7
Complications
There are several complications of haemothorax, which include:2
- Respiratory failure
- Hypovolaemic shock
- Cardiac arrest
There are also complications related to the treatment of a haemothorax:4
- Empyema
- Fibrothorax
- Pneumothorax
- Further worsening of haemothorax
Reviewer
Professor Eleanor Mishra
Consultant in Respiratory Medicine
Editor
Dr Jamie Scriven
References
- Patrini D, Panagiotopoulos N, Pararajasingham J, et al. Etiology and management of spontaneous haemothorax. Journal of Thoracic Disease. 2015. Available from: [LINK].
- Zeiler J, Idell S, Norwood S, et al. Hemothorax: A Review of the Literature. Clinical Pulmonary Medicine. 2020. Available from: [LINK].
- Pohnan R, Blazkova S, Hytych V, et al. Treatment of Hemothorax in the Era of Minimally Invasive Surgery. Military Medical Science Letters. 2019. Available from: [LINK].
- Dogrul BN, Kiliccalan I, Asci ES, et al. Blunt trauma related chest wall and pulmonary injuries: An overview. China Journal of Traumatology. 2020. Available from: [LINK].
- Salim S et al. License: [CC BY 2.0].
- Havelock T, Teoh R, Laws D, et al. Pleural procedures and thoracic ultrasound: British Thoracic Society pleural disease guideline 2010. 2010. Available from: [LINK].
- Higgins MCSS, Shi J, Bader M, et al. Role of Interventional Radiology in the Management of Non-aortic Thoracic Trauma. Seminars in Interventional Radiology. 2022. Available from: [LINK].
Discover more from Bibliobazar Digi Books
Subscribe to get the latest posts sent to your email.